Delivering e-Health therapy to people with traumatic brain injury
Acceptance and Commitment Therapy delivered via video conferencing can improve mental wellbeing in people with traumatic brain injury, shows research from The Ingham Institute for Applied Medical Research.

Traumatic brain injury (TBI) which occurs from a significant blow or hit to the head can have physical, cognitive and emotional changes such as depression, anxiety, anger and stress. People experiencing mental health or psychological distress after TBI often require additional support but may not find it easy to access appropriate services, especially if they live in remote or rural regions. If their head trauma has also caused health concerns such as mobility issues and changes to their vision, dizziness and ability to drive, they may find it challenging at times to leave their home for appointments to see a mental health professional in person.
Mental Health support after traumatic brain injury
To address these healthcare barriers, Dr Diane Whiting developed an e-Health program tailored to people with moderate to severe traumatic brain injury. Whiting is a Project Manager and Research Fellow from the Brain Injury Rehabilitation Research Group. The group is located at the Ingham Institute of Applied Medical Research (IIAMR) and was responsible for conducting the trial into the efficacy of the program.
The aim of this work has been to build evidence about the optimal psychological interventions for moderate to severe traumatic injury. The program which is called ACT-Adjust, focusses on psychological wellbeing and uses a therapeutic approach called Acceptance and Commitment Therapy (ACT) to improve the mental health of individuals after traumatic brain injury.
Infrastructure needs for the research have been supported by a Medical Research Support Program grant. This was awarded by NSW Health’s Office for Health and Medical Research to the Ingham Institute for Applied Medical Research. Funding for the program research, which will run until June 2024, has been provided by an innovation grant from icare, Insurance and Care NSW.
Increasing access to psychological treatment
Compared to those in metropolitan areas, people with TBI in remote and rural regions have more limited mental health services and more limited access to psychologists. In addition, few psychologists have been specially trained in how to adapt psychological interventions to the specific cognitive impairments and mental health challenges impacting people with traumatic brain injury. These may include problems with attention, speed of information processing, memory and executive functions. This means that it can be challenging for people with traumatic brain injury to receive timely, accessible and appropriately targeted therapy. The ACT-Adjust program which involves nine therapy sessions tailored to traumatic brain injury, has been assessing whether delivering this therapy online is equally as beneficial as delivering sessions face to face.
This virtual initiative was prompted by a successful pilot study at Liverpool Hospital in the South Western Sydney Local Health District that provided ACT in person. The program adjusted standard delivery of Acceptance and Commitment Therapy to the needs of people with TBI and found it achieved statistically and clinically significant reductions in depression and stress when compared to an active control group.
On-line versus face-to-face therapy
The option of therapy via eHealth, which involves delivery of healthcare at a distance via technology, has the potential to increase service access, yet little research has examined the effectiveness of providing psychological treatments this way. So, the ACT-Adjust trial set out to compare two different modes of therapy delivery using two groups with an equal number of participants. The participants were randomly selected to receive the program in person or via video conferencing (VC). Both groups were recruited across two metropolitan and six regional community rehabilitation services of the NSW Health Agency for Clinical Innovation Brain Injury Rehabilitation Network. All of the participants had experienced moderate to severe traumatic brain injury, with clinically significant levels of psychological distress.
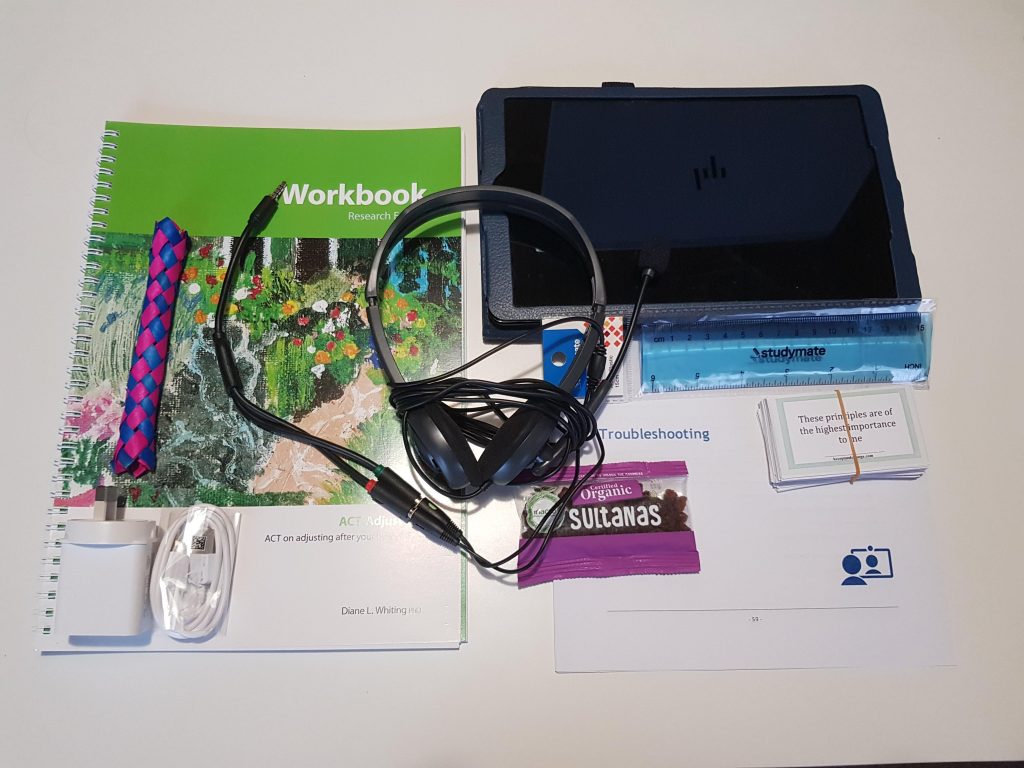
The video conferencing group received their therapy intervention through a platform called Health Direct Video Call. They were also provided with therapy materials (a tablet device) and charging equipment with a prepaid data SIM (4G where possible). Prior to commencement of treatment, a research assistant for the project conducted a technology home visit. During the visit the assistant delivered the kit of therapy materials, the video conferencing equipment and training on how to use it. They also completed a test run using the VC platform. The ‘in person’ group received face to face therapy via individual sessions with a psychologist or mental health accredited social worker. They were also supplied with therapy support materials.
Program participation prompts
During the 13 weeks of the program, automated text messages were sent to all of the participants for appointment reminders and between-session home task reminders. Following informed consent, measures of mental health and wellbeing were taken. These were recorded by the clinician delivering the intervention prior to randomisation of the two groups and also when commencing the program. These measures were then taken again at the end of the program and three months later, by a ‘blinded assessor’, which means the assessor had no knowledge of who was in which group. The Depression Anxiety and Stress Scale (DASS-21) was the primary outcome measure. The study hypothesis was that outcomes from the video conferencing delivery would be no different to outcomes from the face-to-face counselling.
Benefits of Acceptance and Commitment Therapy
Acceptance and Commitment Therapy is a third wave cognitive behavioural therapy and implements mindfulness and other techniques which assist people to improve their psychological flexibility. Rather than focusing on avoiding or getting rid of unwanted and difficult emotions and thoughts, Acceptance and Commitment Therapy encourages people to be more accepting of them. This involves the adoption of different self-help tools to deflect and distance from unpleasant and painful thoughts and feelings. Those approaches include a range of techniques such as viewing your emotions from a distance, as though you are a scientist, or imagining you are placing these thoughts in your cupped hands and creating a physical image of the thought (physicalizing the thought). These approaches help to reduce the power of unpleasant and painful thoughts or memories. In addition, people learning Acceptance and Commitment Therapy are encouraged to engage in activities and actions consistent with their values. In the context of the ACT-Adjust program this helps them achieve a more meaningful and satisfying life despite their TBI.
Study findings
This research confirms the promising potential of video conferencing as a viable and effective mode for delivering psychological interventions, specifically the ACT-Adjust program, to support people with mental health distress after a moderate to severe traumatic brain injury. Early findings show that participants in both groups reported the same pattern of treatment effects indicating improvements pre and post intervention, which were maintained at a three month follow up. These improvements have occurred in primary and secondary outcome variables including psychological distress, experiential avoidance, quality of life, engaged living and satisfaction with life.
No significant differences were found between those who received face-to-face ACT therapy compared with those receiving video conference delivery. These similar results suggest that using technology can help break down distance barriers ensuring that effective mental health support is more accessible to everyone. Participants in the face to face and video conferencing groups also provided qualitative data. They reported their adoption of strategies acquired through participation in the ACT-Adjust program, including mindfulness, defusion (detaching and distancing) and committed action based on values.
Given the positive results of the Act-Adjust trial, Dr Whiting is now running training workshops to build capacity among psychologists and other mental health workers in the delivery of ACT-Adjust, both through eHealth and face to face modalities, to better improve the mental health of people living with moderate to severe traumatic brain injury.
Updated 1 year ago